
Recently, our team performed transcatheter edge-to-edge repair (TEER) procedures using the V-Clamp device in two dogs — one with stage C and another with stage D myxomatous mitral valve disease (MMVD). These cases mark the third and fourth TEER procedures performed in Malaysia.
What is TEER and V-clamp?
TEER stands for transcatheter edge-to-edge repair. It is a hybrid minimally invasive procedure used to treat MMVD by clipping or grasping the mitral valve leaflets together via a catheter, thereby reducing leakage without open-heart surgery.
The V-Clamp is the name of the device for performing TEER in dogs.
Why TEER?
This is because MMVD ultimately remains a surgical condition.
Open-heart surgery to repair the mitral valve is currently unavailable in Malaysia.
While medical therapy can help control symptoms and delay disease progression, it does not cure the underlying valve degeneration. Once a dog enters congestive heart failure, the prognosis is typically limited to only a few months despite optimal medical management.
Meet Mango:
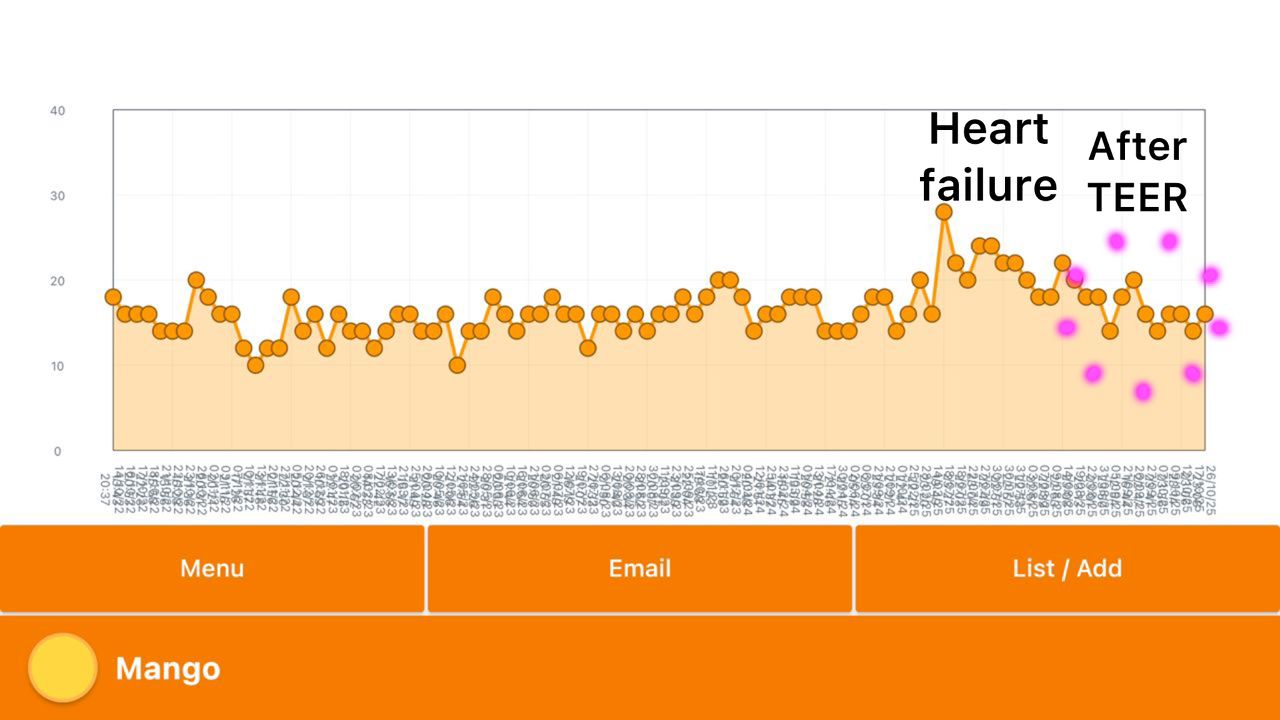
Mango is an 11-year-old Shetland Sheepdog, sadly succumbed to heart failure secondary to MMVD in July 2025.

What happened to Mango?
The surgery was successful despite procedural complications and relentless pressure bore down on the entire team. What followed was a sleepless night of ICU monitoring that left me utterly drained. Through the ICU night, I remained on standby, ready to respond to the nurse at any time.
How is Mango now?
Currently Mango’s sleeping respiratory rate has stabilized at 14–16 bpm. She’s more active, requires less diuretic, and her ACE inhibitor has been discontinued since the surgery. Seeing her regain energy and comfort has made every hardship worthwhile.
Meet Petunia:
Petunia is an 11-year-old little warrior with stage D (end-stage) MMVD. She had already reached the limits of medication, with kidney dysfunction and a heart that’s been fighting bravely for months.

What happened to Petunia?
Before the procedure, I spoke honestly with her owner about the extremely high risk involved. Yet, with love and hope, she chose to give Petunia this final chance.
Not only that — the anesthetic risk in this patient with cardiorenal syndrome was significant, but my incredible anesthesia team stood strong through every moment.
Her heart’s orientation was far from normal, making it a real challenge to find the right puncture site. But with patience, teamwork, and faith, we made it through.
How is Petunia now?
One week after surgery, Petunia receives a lower dosage of diuretic medication. Her sleeping respiratory rate remains around 24 bpm.
During the first few days, she showed little interest in food, but she has since regained her appetite and continues to recover steadily.
Sometimes I wonder why we choose such a difficult path, driving ourselves to the edge of exhaustion. As my assistant candidly pointed out, the effort doesn’t even tally with the profit.
But this is the reality of the learning curve: steep, unforgiving, and exhausting. Perhaps it is by walking this hardest road that we truly grow, not only as clinicians but as a team.

